
People usually search for this











Tirzepatide: Dual Incretin Mechanism and What the Clinical Evidence Shows
Tirzepatide differs from most of the molecules discussed in this section. This is because it is no longer an investigational peptide in a regulatory gray area, but rather an FDA-approved drug marketed under the brand names Mounjaro (for the treatment of type 2 diabetes) and Zepbound (for weight management). It has a completed clinical trial program, approved prescribing information, and a growing post-marketing database.
That is precisely why the discussion surrounding this peptide is different, because we can rely on real clinical data and observations. Let’s take a closer look at what it is, how it works, and, most importantly, why.
⚠️ Tirzepatide is an approved prescription drug. This material is for educational purposes only and does not constitute medical advice. Questions regarding its use, dosage selection, and the appropriateness of therapy are to be determined by the treating physician.
What Makes Tirzepatide Different: The Dual Agonist Mechanism
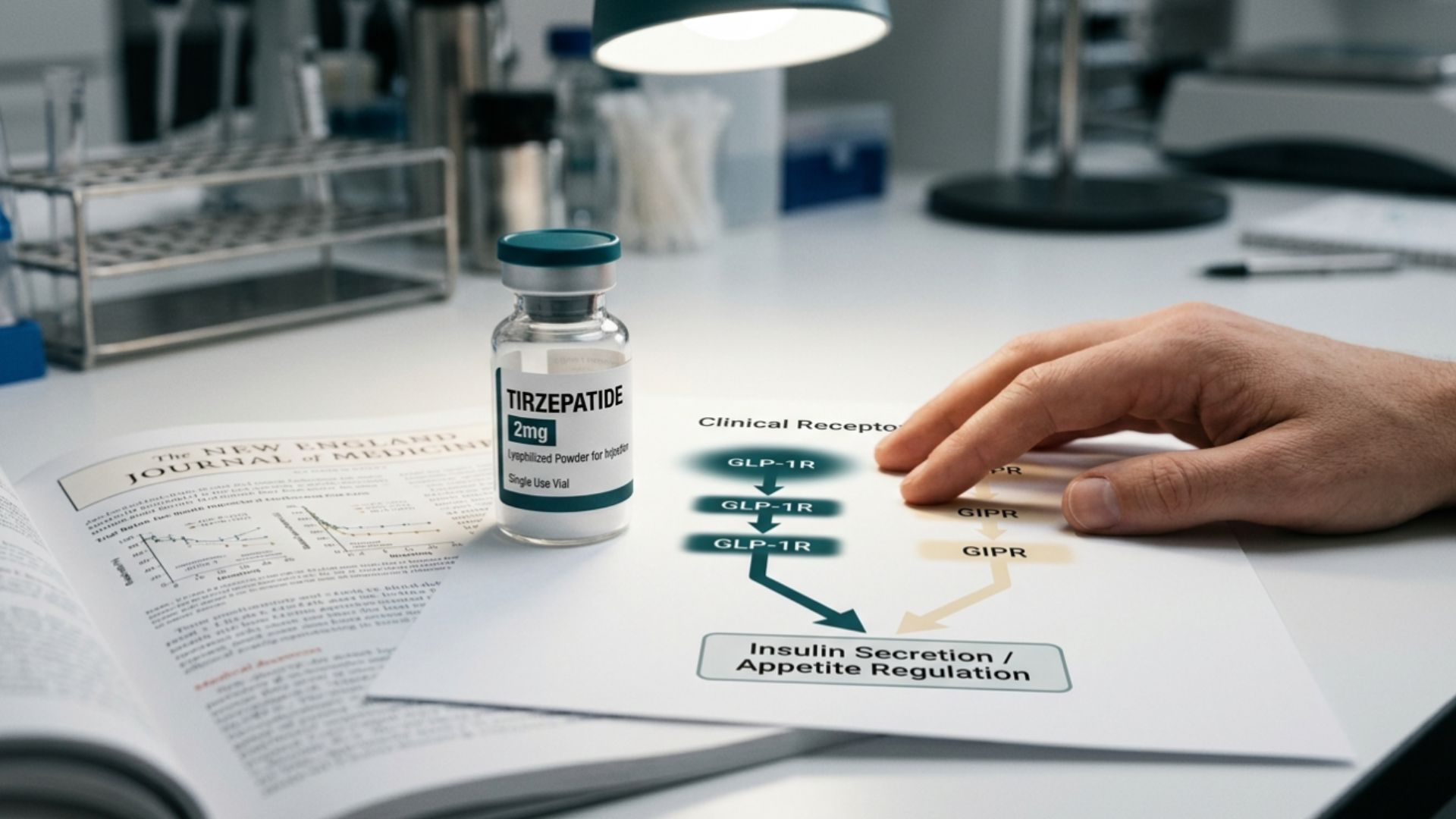
To understand why tirzepatide has attracted so much attention, we need to start with its mechanism of action. Most previous drugs in this class were agonists of a single receptor: GLP-1 (glucagon-like peptide-1). You may have heard of such peptide-based treatments under the name semaglutide. But tirzepatide is a dual agonist: it simultaneously activates both GLP-1 and GIP (glucose-dependent insulinotropic polypeptide) receptors.
Both of these hormones are incretins – peptides produced by the gut in response to food intake. GLP-1 has long been known as a therapeutic target for diabetes and obesity: it stimulates insulin secretion, inhibits glucagon secretion, slows gastric emptying, and reduces appetite. GIP remained largely overlooked for a long time: in the context of obesity, its insulinotropic effect is reduced. However, studies have shown that the GIP receptor is widely expressed in adipose tissue and the central nervous system, and that simultaneous activation of the GIP and GLP-1 pathways produces a different metabolic profile than stimulation of either pathway alone.
This was precisely the hypothesis tested by the SURPASS clinical program.
Tirzepatide vs. Semaglutide: What the Comparative Trial Data Shows
The most direct answer to the question of tirzepatide vs. semaglutide remains the SURPASS-2 trial, a randomized, open-label Phase 3 study, whose results were published in the New England Journal of Medicine in 2021.
The study included 1,879 participants with type 2 diabetes who were taking metformin. They were randomized to three doses of tirzepatide and a semaglutide 1 mg group for 40 weeks.
The primary endpoints were changes in HbA1c and body weight from baseline.
On both measures, all three tirzepatide doses statistically significantly outperformed semaglutide 1 mg. The context is important: Semaglutide was administered at a dose of 1 mg, the maximum dose approved for the treatment of diabetes at the time of the trial. This is a direct, rather than an indirect, comparison, which increases its evidential strength.
However, one cannot conclude from these data that “tirzepatide is always better than semaglutide” in an absolute sense. The trial was conducted in a specific population, with specific parameters and endpoints. In real life, however, all patients are different and have different comorbidities. These are all clinical variables that a doctor takes into account, rather than the trial’s population-level data.
Retatrutide vs. Tirzepatide: The Next Step in Receptor Agonism
If tirzepatide represents a step from one receptor to two, then retatrutide vs. tirzepatide is a discussion of the next level: triple agonism. Retatrutide adds the glucagon receptor (GCGR) to the GLP-1R and GIPR, which, in theory, enhances the lipolytic component through direct action on adipose tissue.
But when discussing the “triple-action” of retatrutide, it’s essential to mention an important factor. The FDA has approved Tirzepatide; retatrutide has not. The fact is that research is still ongoing. Retatrutide has completed Phase 2 trials, the data from which were published in the NEJM in 2023 and generated significant research interest. As of this writing, Phase 3 trials are underway, but these are still research studies, meaning regulatory approval is still a long way off.

Tirzepatide Weight Loss: What SURMOUNT-1 Actually Found
A separate issue that deserves its own analysis is tirzepatide weight loss in the context of the trial involving people with obesity who do not have type 2 diabetes. After all, when people search for this peptide online, they are most often interested specifically in weight loss.
SURMOUNT-1 was a randomized, double-blind, placebo-controlled Phase 3 trial involving 2,539 participants who were obese or overweight. All participants received tirzepatide or a placebo for 72 weeks in combination with a reduced-calorie diet and increased physical activity. The results were published in the NEJM in 2022.
Participants receiving tirzepatide experienced a dose-dependent reduction in body weight, ranging from 16.0% to 22.5% of baseline in different dosing groups. Important details that are often omitted in summaries:
- All participants followed a calorie-restricted diet and were physically active (this was an integral part of the protocol).
- The trial studied a specific population; the results are not automatically applicable to all people with any BMI.
- The authors themselves described the observed degree of weight loss as “unusually pronounced” compared with previously available medications.
Tirzepatide Side Effects: What the Label and Trial Data Report
The discussion of tirzepatide side effects is based on real, approved data, which sets it apart from many investigational compounds. And unfortunately, there are indeed side effects.
The most commonly reported adverse events in the SURPASS and SURMOUNT trials:
- Gastrointestinal effects: nausea, diarrhea, vomiting, constipation, and decreased appetite are the most common (especially in the early stages).
- Injection-site reactions.
- Transient changes in heart rate.
Several safety concerns that are regularly discussed in the medical literature and reflected in the approved prescribing information:
- Risk of medullary thyroid carcinoma; contraindicated in individuals with a personal or family history of this disease or MEN 2; based on data from animal models.
- Pancreatitis is a rare but documented risk that warrants attention when risk factors are present.
- Changes in vision in patients with diabetic retinopathy following rapid improvement in glycemic control.
- Post-marketing surveillance is ongoing: some long-term safety issues, including cardiovascular outcomes, are being clarified in ongoing trials.
Microdosing Tirzepatide: Why This Is a Prescriber’s Decision
The term microdosing tirzepatide is becoming increasingly common, primarily in longevity and biohacking communities. The rationale typically cited by proponents of this approach is that subtherapeutic doses may provide some of the metabolic effects with better tolerability. The scientific interest in this issue is understandable – the pharmacodynamics of the drug at subtherapeutic concentrations are indeed poorly understood.
However, it is necessary to draw a fundamental distinction here. Tirzepatide is a prescription drug with an approved titration regimen developed based on clinical data. Any deviation from this regimen (including the use of doses lower than those approved) is a medical decision requiring a clinical assessment of the individual patient. This involves considerations of pharmacokinetics, contraindications, comorbidities, and medical monitoring.
The dosing regimen for tirzepatide is determined solely by a licensed physician. This is particularly relevant for compounded versions of the drug, which may differ significantly in composition and concentration from the approved original.
Key Takeaways
Tirzepatide is an approved prescription drug with one of the most extensive clinical programs in the incretin agonist class.
A few points that accurately summarize its place in evidence-based medicine:
- Dual GIP/GLP-1 agonism represents a fundamental mechanistic advancement over GLP-1 monotherapy; the SURPASS-2 trial demonstrated statistically significant advantages over semaglutide 1 mg in a specific population.
- SURMOUNT-1 documented a marked reduction in body weight in obese individuals under a controlled protocol.
- The adverse event profile is based on real-world clinical data from large randomized trials (not on preclinical observations).
- Retatrutide, as the next level of receptor coverage, is currently in the trial phase and is not yet a clinical option.
Any questions related to use – indications, treatment regimen, compatibility with other medications, monitoring – are solely within the physician’s purview. In the Grey Research Peptides catalog, Tirzepatide is available for in vitro laboratory use by qualified professionals.