
People usually search for this











Metabolic Research Peptides: From Semaglutide to Retatrutide – The Mechanism Behind the Demand
Metabolic peptides are perhaps the most talked-about topic in pharmacology right now – both in scientific journals and far beyond. Some are already being used in clinical practice as prescription drugs, while others are still in the testing phase. But there is a third category: peptides that are studied only at the mechanistic level.
We prepared this material to explain the mechanisms and how a single discovery sparked a wave of molecules, each more complex than the last. Tirzepatide, retatrutide, semaglutide, and cagrilintide – all of these are part of the same story. We will try to tell it honestly.
⚠️ This material is intended solely for educational purposes. Some of the compounds mentioned are approved prescription drugs, while others are experimental compounds currently in clinical trials. Nothing in this text constitutes medical advice and should not be used as a basis for self-medication. Consult a doctor with any clinical questions.
The Mechanism: GLP-1, GIP, Glucagon, and Amylin
To understand why these molecules exist at all, we need to examine four receptor systems. These are the foundations of this entire field:
- GLP-1 (glucagon-like peptide-1). This is an incretin released by the intestines in response to food intake. It activates the GLP-1R, stimulates insulin secretion, inhibits glucagon secretion, slows gastric emptying, and affects satiety centers in the brain. This was the starting point for the entire field.
- GIP (glucose-dependent insulinotropic polypeptide). This is the second incretin, also secreted by the intestine. It remained virtually unnoticed for a long time until it was discovered that its receptor, GIPR, is widely present in adipose tissue and the CNS. The combined activation of GIP and GLP-1 receptors yields a different metabolic profile than each pathway acting separately.
- Glucagon receptor (GCGR). Glucagon might appear to be an antagonist of the entire system – it raises blood glucose levels. However, in adipose tissue, its activation enhances lipolysis, making it an interesting target, particularly when combined with GLP-1.
- Amylin. This is a peptide hormone co-secreted by the pancreas along with insulin. It plays a role in regulating satiety, gastric emptying rate, and postprandial hyperglycemia.
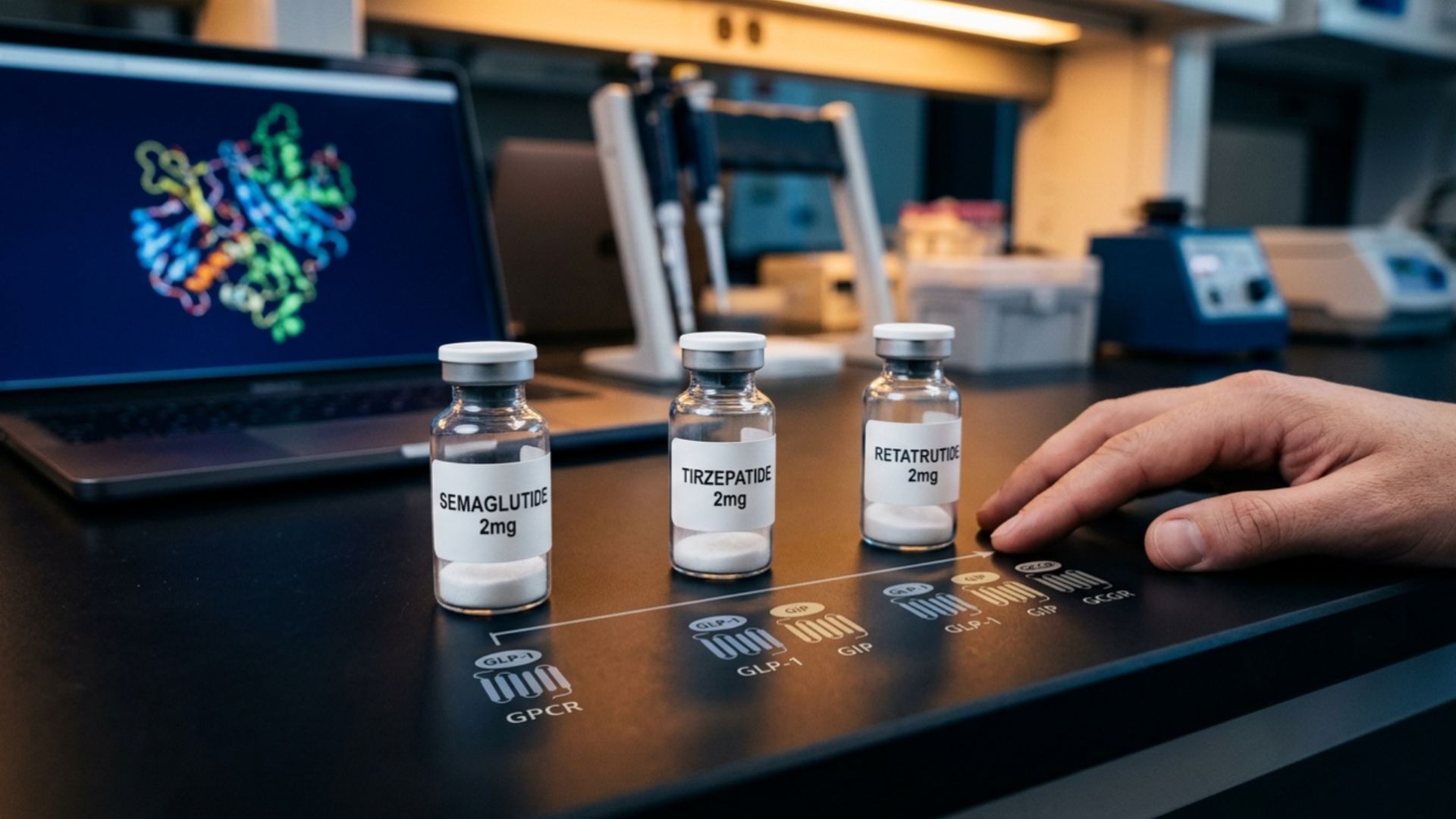
From Single to Multi-Receptor Agonists
The evolution of the class is quite clear, from simple to complex.
- Semaglutide is a GLP-1R agonist. One receptor, one mechanism. It is with this compound that the STEP and SELECT trials are associated, trials that set the benchmark for the entire field. Against this backdrop, the comparison of tirzepatide vs. semaglutide became the first major test of what adding a second target provides.
- Tirzepatide is a dual GIP/GLP-1 agonist. Its direct comparison with semaglutide in the SURPASS-2 trial, published in the New England Journal of Medicine, showed statistically significant differences across several metabolic parameters (Frías et al., NEJM, 2021). Important: these are data from a specific trial in a specific population – extrapolate them with caution.
- Retatrutide is a triple agonism. Retatrutide is the next step, adding glucagon receptor activation to GLP-1R and GIPR. At this time, the peptide is still in the clinical trial phase. Phase 3 trial data have shown significant results, but this drug is still experimental and has not been approved in any jurisdiction.
Retatrutide vs. Tirzepatide
People looking to lose weight often come across comparisons of retatrutide vs. tirzepatide. From a scientific standpoint, this is not simply a comparison of two molecules. It is a comparison of an approved drug with an experimental compound in the testing phase.
Tirzepatide is FDA-approved; retatrutide is not. Not in the U.S., not in the EU, absolutely nowhere. Phase 3 trials are already in progress. But this is not the end yet. There is still a lot of work to be done before regulatory approval, and the results are unpredictable.

Retatrutide: What the Investigational Research Shows
Retatrutide peptide (a triple agonist of GLP-1R/GIPR/GCGR) is the most mechanistically complex compound in this review, and that is precisely why it is receiving so much attention.
The logic behind triple agonism: GLP-1 and GIP act on insulin sensitivity and satiety, while the glucagon component adds a direct effect on lipolysis in adipose tissue. In theory, this allows for simultaneous modulation of metabolism through three independent pathways.
Phase 3 data showed significant changes in metabolic parameters among participants – attracting interest both within the scientific community and beyond.
It is important to note honestly:
- Phase 3 does not constitute proof of clinical efficacy and safety in the general population.
- Long-term safety data in humans are currently limited.
- Approval is a separate process that can take years and is not guaranteed.
Retatrutide is listed in our catalog as a research compound: Retatrutide 15mg for research use only.
Where Cagrilintide Fits
Cagrilintide is a slightly different story because it is an amylin analog, not an incretin.
Amylin is secreted by the pancreas alongside insulin and helps regulate satiety and postprandial glycemia via distinct receptors. Cagrilintide is being developed as a long-acting amylin analog and is being studied in combination with semaglutide under the name CagriSema. It is this combination that interests researchers: GLP-1R agonism plus the amylin pathway are two fundamentally different mechanisms working in parallel.
A trial published in The Lancet in 2021 presented data on cagrilintide as monotherapy and in combination (Enebo et al., The Lancet, 2021). The compound remains experimental. In our catalog, it is available as Cagrilintide/Semaglutide Blend for laboratory use.
“The Demand”: Research Interest vs. Medical Reality
The word “demand” as it applies to these molecules should be interpreted with caution.
Interest in them is enormous, and this is understandable. Metabolic diseases, obesity, and insulin resistance are all real problems that are very difficult to overcome. And when clinical trials show significant changes in metabolic parameters, these findings are noticed far beyond the pages of scientific journals. This creates a situation where the line between “the drug is being studied” and “the drug is available” begins to blur in the public’s perception.
The reality is as follows:
- Tirzepatide is an approved prescription drug. It is used under a doctor’s supervision for specific indications. Self-use is prohibited.
- Retatrutide is an experimental compound currently undergoing trials. It is not approved. It is not an available treatment option.
- Cagrilintide is also an experimental compound. Trials are ongoing; there is no approval.
Research interest in the class is not an indicator that the compounds are ready for use outside of clinical settings. These are two completely different matters.
Key Takeaways and Safety
If we put it all together into a single picture.
Progress in the class reflects genuine research logic: each addition of a mechanism addressed a specific scientific question about metabolic pathways. This is not a marketing escalation; it is an accumulation of biological understanding. Although the line between the two is often blurred in the public sphere.
Status Map:
- Semaglutide and tirzepatide – approved drugs with indications, used under medical supervision
- Retatrutide and cagrilintide – experimental; insufficient data on long-term safety in humans
For experimental compounds, it is particularly important to note that the lack of approval is not a mere formality. It signifies the absence of a confirmed safety profile in a sufficiently large population. Phase 2 and 3 trials answer some questions and raise others; they do not conclusively resolve the issue.
Any practical questions (selection, applicability, suitability for an individual situation) should be directed exclusively to a physician.
In the Grey Research Peptides catalog, compounds in this class are available for laboratory use: Tirzepatide, Retatrutide, Semaglutide, and Cagrilintide/Semaglutide Blend. Exclusively for in vitro research by qualified professionals. Not for use in humans or animals.